



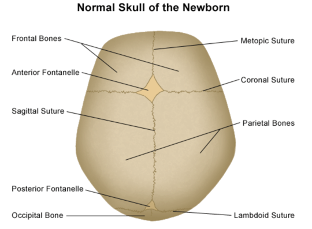
The infant’s skull is composed of bony plates separated by sutures. As the baby grows, the calvarium deposits new bone along suture lines in response to the rapidly growing brain. During the first two years after birth, the brain increases in size up to 75% of its adult volume.
Craniosynostosis is the premature fusion of one or more cranial sutures and it effects 1 in every 2500 births worldwide. As a result of the premature fusion, the skull is restricted in its growth and cannot grow evenly in all directions. In most cases, craniosynostosis involving one suture occurs sporadically and is an isolated defect. However, this abnormality is more likely to occur in multiple pregnancies or if there is uterus abnormality like bicornuate uterus. Craniosynostosis could be identified in patients with autosomal dominant syndromes likes Apert’s, Crouzon’s, and Pfeiffer’s syndrome. In this case, mutations occurs in the fibroblast growth factor receptor (FGFR).
TYPES
 There are 4 different types of cranial deformities: scaphocephaly, plagiocephaly, trigonocephaly, and acrocephaly.
There are 4 different types of cranial deformities: scaphocephaly, plagiocephaly, trigonocephaly, and acrocephaly.
Scaphocephaly – most common type. Premature fusion of the sagittal suture results in long cranium and decreased width.
Plagiocephaly – premature closure of coronal or lambdoidal sutures unilaterally or bilaterally and is second most common type. If coronal suture is affected, then forehead looks flat and eyebrows are elevated on the affected side or both. In case of lambdoid suture closure, back of the head is flat, forehead is set back, and ear on the affected side is low.

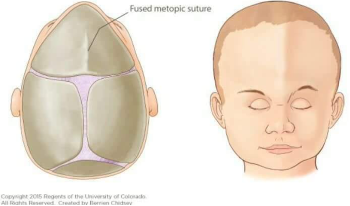
Trigonocephaly – premature fusion of metopic suture and is the second least common case. It is characterized by a narrow, triangle-shaped forehead with a prominent midline ridge and superior-lateral orbital depression.
Acrocephaly – is where sagittal, coronal, and lambdoid sutures fuse prematurely and is the rarest abnormality. The anterior cranium is elevated compared to posterior resulting in a slant. This is seen in Crouzon or Apert syndromes.
DIAGNOSIS
Diagnosis is initially based on physical exam, followed by a x-ray or CT to identify the specific abnormality. CT is a better test that assesses the extent of fusion and its effect on surrounding bones.
DIFFERENTIAL DIAGNOSIS
Positional flattening (positional plagiocephaly) – flattening of the back of the head due to supine sleeping position to prevent sudden infant death syndrome. This is easily confused with plagiocephaly. To distinguish between the two, look for parallelogram shape head on posterior view in patients with plagiocephaly or perform x-ray. Positional flattening can be treated by change in positioning and a custom-fitted cranial molding orthosis (helmet).
Brachycephaly –Can look like positional flattening and plagiocephaly because presents as flat back of head. Brachycephaly results from bilateral coronal synostosis.
Torticollis – tight sternocleidomastoid muscle on one side of the neck, causes the baby to hold its head to one side. This results in flattening of the head on the side of the tight muscle.
COMPLICATIONS
- Increased intracranial pressure (ICP) and inhibition of brain growth
- Possible impairment in cognitive and neurodevelopmental function such as developmental delay, poor feeding, and weight gain
- Deficits in vision, hearing, and speech due to cranial nerve involvement
- Poor self-esteem and social isolation due to abnormal appearance
MANAGEMENT
Patient care should be referred to craniofacial team for evaluation or physician with craniofacial training such as a plastic surgeon or neurosurgeon. Surgical repair of craniosynostosis prevents increase in intracranial pressure. It is recommended to perform surgery before 1 year of age. The best time to perform open surgery is between 9 and 12 months to prevent postoperative regression of cranial bones. Surgery can also be performed endoscopically, which requires a smaller incision. Endoscopic surgery can be performed as early as 3 months of age.
Works Cited:
- Edward P Buchnan. (2021) Overview of Craniosynostosis. In: UpToDate, L. E. Weisman & H. V. Firth (Eds.), UpToDate. (Accessed on October 5 2021.)
- https://healthproadvice.com/kids/Cranial-Helmet-Therapy-for-Babies-Does-It-Actually-Fix-a-Flat-Head
- https://www.stanfordchildrens.org/en/topic/default?id=anatomy-of-the-newborn-skull-90-P01840